
What is the mitral valve?
The heart has four chambers, the left atrium (LA), left ventricle (LV), the right atrium (RA) and right ventricle (RV). The heart also has four valves which helps maintain a forward flow of blood amongst these chambers and prevents backward flow of blood. The valves are the Mitral valve, Tricuspid valve, Aortic valve and the Pulmonary valve. Mitral valve is a valve located between the left atrium and left ventricle of the heart. It has two leaflets resembling a priest’s mitre or cap. The function of the mitral valve is to open and allow forward flow of blood from the LA to LV when the LV relaxes and to close and prevent back-flow into the LA when the LV contracts to pump blood into the aorta.
What is mitral stenosis and what causes it?
Mitral stenosis is a condition affecting the mitral valve where the valve gets thickened. Mitral stenosis occurs commonly due to a condition called Rheumatic heart disease. In this condition, as a reaction to a childhood throat infection by a bacteria called Beta Hemolytic Streptococci, the mitral valve undergoes progressive thickening and narrowing. This causes resistance to forward flow of blood from LA to LV thus causing pressure to build up inside the LA.
What are the symptoms of mitral stenosis? The progressive thickening of the valve results in a progressive obstruction to forward flow of blood across the valve thereby resulting in a build-up of back pressure in the chamber behind the valve, which is the LA and then inside the lungs just as in a pressure cooker with a dysfunctional valve. The increased pressure causes blood and fluid to leak into the lungs and thus preventing effective air entry into the lungs and oxygen exchange. This causes breathing difficulty while walking, bathing and performing day to day activities. In advanced cases of mitral stenosis, breathing difficulty can occur at rest also. When left untreated it can also cause the LA to become enlarged and can cause clot formation inside it which can get dislodged into the brain leading to stroke or paralysis.
What are the treatment options for mitral stenosis?The treatment for this condition may be open heart surgery and replacement of the valve with a metal valve or tissue valve or a procedure without open heart surgery called Percutaneous Trans-venous Mitral Commissurotomy (PTMC) which is also called Balloon Mitral Valvotomy (BMV).
What is Percutaneous Trans-venous Mitral Commissurotomy (PTMC) or Balloon Mitral Valvotomy (BMV)?
Percutaneous Trans-venous Mitral Commissurotomy (PTMC) or Balloon Mitral Valvotomy (BMV) is a procedure where a balloon called the Inoue balloon is placed across the mitral valve and the inflation of this balloon with liquid contrast or dye causes the balloon to split open the mouth of the mitral valve or the commissures. The balloon has three segments. A distal segment which gets inflated first, a proximal segment which gets inflated next and then a waist which inflates last to split or tear the mitral valve commissures and thus opening up the narrowed valve. (Watch video below)
Why is PTMC and not open heart surgery or mitral valve replacement not the preferred treatment for rheumatic mitral stenosis?
The general principle is to delay open heart surgical valve replacement as much as possible as surgical replacement often requires the placement of a metal-valve and may require the patient to take life-long blood thinners or oral anti-coagulants. This puts the patient at a perpetual risk of bleeding and complicating any other non-cardiac surgical procedures he may need in his lifetime. In addition there is also the risk of life threatening bleeding in case of any trauma or accidents. Also there is the risk of the valve getting blocked suddenly by a blood clot and paralysis or stroke, if the blood-thinning medications are not taken on time or missed.
How is Percutaneous Trans-venous Mitral Commissurotomy (PTMC) performed?
Procedure and technique:
The Mitral Valve is located on the Left side of the heart and cannot be approached from the left side of the heart as the balloon can damage the aortic valve and the coronary arteries. Therefore the mitral valve van be reached only from the right side of the heart. The femoral vein in the leg is connected to a vein called the inferior venacava which is connected to the RA of the heart. The entire procedure of PTMC involves delivering the Inoue balloon from the leg to the RA of the heart and then entering the LA through a hole made in the wall between the RA and LA and then across the mitral valve.
The first step involves delivering local anaesthesia over the skin over the femoral vein in the groin region of the leg. Thereafter a pin-hole puncture is made with a needle over the skin to enter the femoral vein. Thereafter a small tube or sheath around 2 mm in diameter is placed inside the femoral vein. Then a wire is passed through this sheath into the RA through the IVC. Then a larger sheath called the Mullin’s sheath is advanced over this wire and the wire is then replaced with a long and sharp needle called the Brockenbrough (BRK) needle. (See Image)

Then a hole is made in the inter-atrial septum or the wall separating the RA and the LA with the BRK needle, a step which is called the septal-puncture (See image). This is the most crucial step in the procedure because the puncture has to be made exactly on a specified spot called fossa-ovalis in the IAS. A puncture anywhere else can cause bleeding towards outside of the heart causing a life threatening condition called cardiac-tamponade.

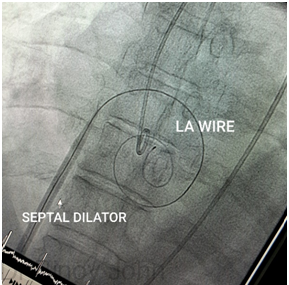
Once the puncture has been made into the LA, a wire called the LA wire, is passed into it and then the hole is made larger with a septal-dilator, to enable the larger balloon to move freely across the hole into the LA.
Thereafter, the balloon is passed across the mitral valve into the chamber beyond the LA called the left ventricle or LV.
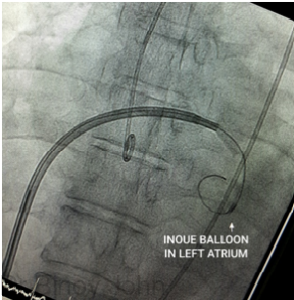
Thereafter the Inoue balloon is threaded over the LA wire to enter the LA. (See image)
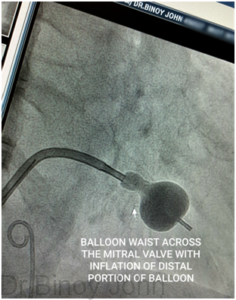
Then from the LA the balloon is crossed across the mitral valve into the LV and the balloon is positioned across the mitral valve commissure. Thereafter the inflation of the balloon with radio-opaque contrast liquid causes the proximal segment of the balloon to get inflated first. Radio-opaque contrast is used so that the balloon can be visible during the procedure. (See image)
With further inflation with contrast the proximal portion of the balloon opens up. (See image)
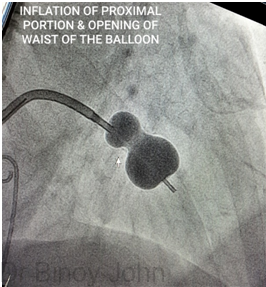
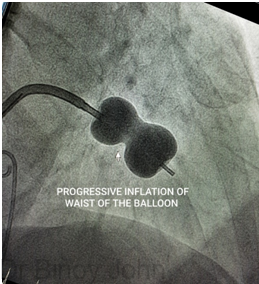
Progressive inflation with contrast causes further opening of the proximal segment of the balloon and the waist of the balloon. (See image)
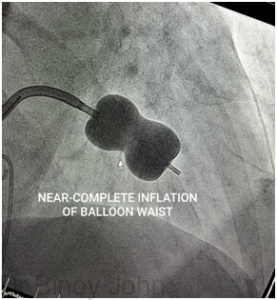
Further inflation causes the near complete opening of the waist (See image)
and finally complete opening of the waist of the balloon to complete the splitting open of the thickened and narrow mitral valve mouth or orifice, (See image)
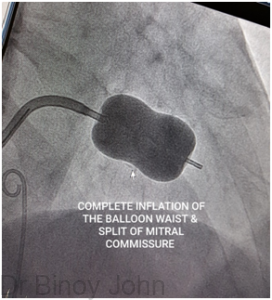
thus completing the procedure. Thereafter the balloon is removed and the puncture site or hole in the femoral vein and leg are closed with pressure and a pressure bandage is applied. The patient is usually discharged the following day after examination of the wound site, an electrocardiogram and an echocardiogram.
This procedure usually gives an excellent result which allows the patient to be free of symptoms and complications for an average of 5 to 10 years and thus be free from the problems and complications that can arise from a surgical placement of a metal valve. However a PTMC may not be possible in all cases of mitral stenosis and such cases can be treated only by open heart surgery and surgical valve replacement.
Also, it is important to note that PTMC is not free of risks and complications either and has a small percentage risk of death, bleeding from the heart and sudden leakage from the valve which may require emergency surgery. But generally, in the hands of a skilled and experienced interventional cardiologist such risks are lower.
Watch Video:
Watch Video: Re-do Percutaneous Transvemous Mitral commissurotomy.
Expertise: Dr Binoy John is highly experienced with valve interventions with over a thousand procedures in various high risk and very complex subsets including percutaneous trans-venous mitral commissurotomy in term pregnant women and elderly patients. He is an invited speaker in international and national conferences to give ‘Tips and tricks’ lectures on the same. His cases of PTMC in pregnancy has been presented in the world’s biggest interventional conference Trans-Catheter Therapeutics 2024, Washington in the Challenging cases- Masters session.
Video: Talk at TCT 2024 Washington on PTMC in Term Pregnancy





