
What is Rotablation angioplasty and who needs it?
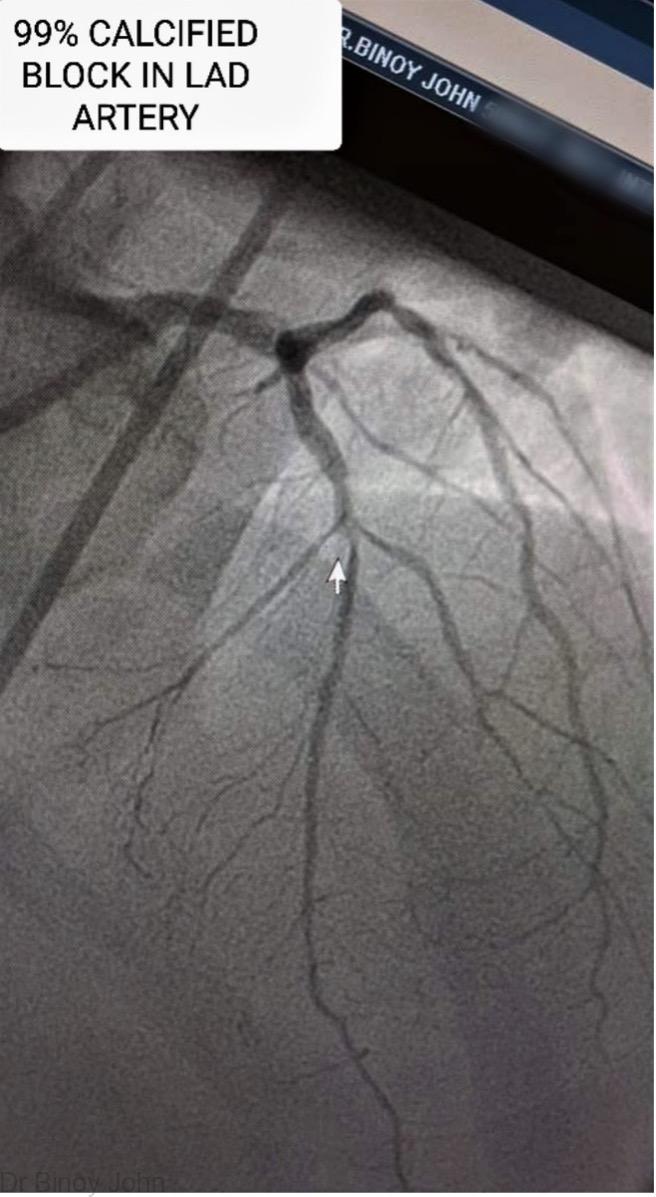
The function of the heart is to pump blood to different parts of the body. For the heart to function as an effective pump it needs energy, which is supplied to it via three arteries which run on its surface, called the coronary arteries. The coronary arteries have an average diameter of 2 to 4 mm. When a significant block or stenosis develops inside a coronary artery, the blood supply to the heart gets compromised and is not able to supply the energy or oxygen demand of the heart. This can classically result in chest pain (angina) on exertion or at rest depending on the severity of the block.
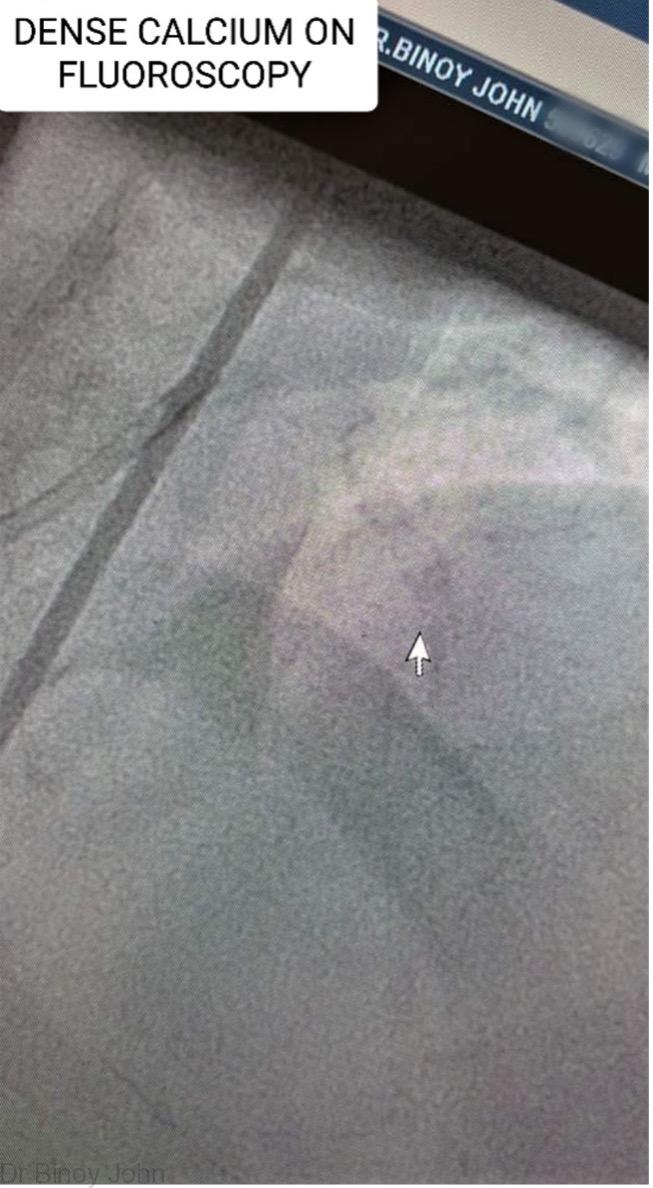
A block is essentially made of fat or lipids and usually develops over time by a process called atherosclerosis. Majority of these fat filled blocks are soft and can easily be opened with a regular angioplasty balloon. But however, some blocks may accumulate calcium deposits in it over time, which can make the blocks hard as a stone. These blocks naturally, because of their hard consistency do not give way to regular angioplasty balloons. Often, they result in rupture of the balloons and may cause vessel injury and can complicate the situation. Thus calcified blocks need an angioplasty different from the conventional one and is called Rotablation angioplasty or Rotational atherectomy or Percutaneous Transluminal Rotational Atherectomy (PTRA).
What are the other techniques available to open calcified blocks?
Other techniques include Intra-Vascular Lithotripsy (IVL) and Orbital Atherectomy
What is Rotablation angioplasty?
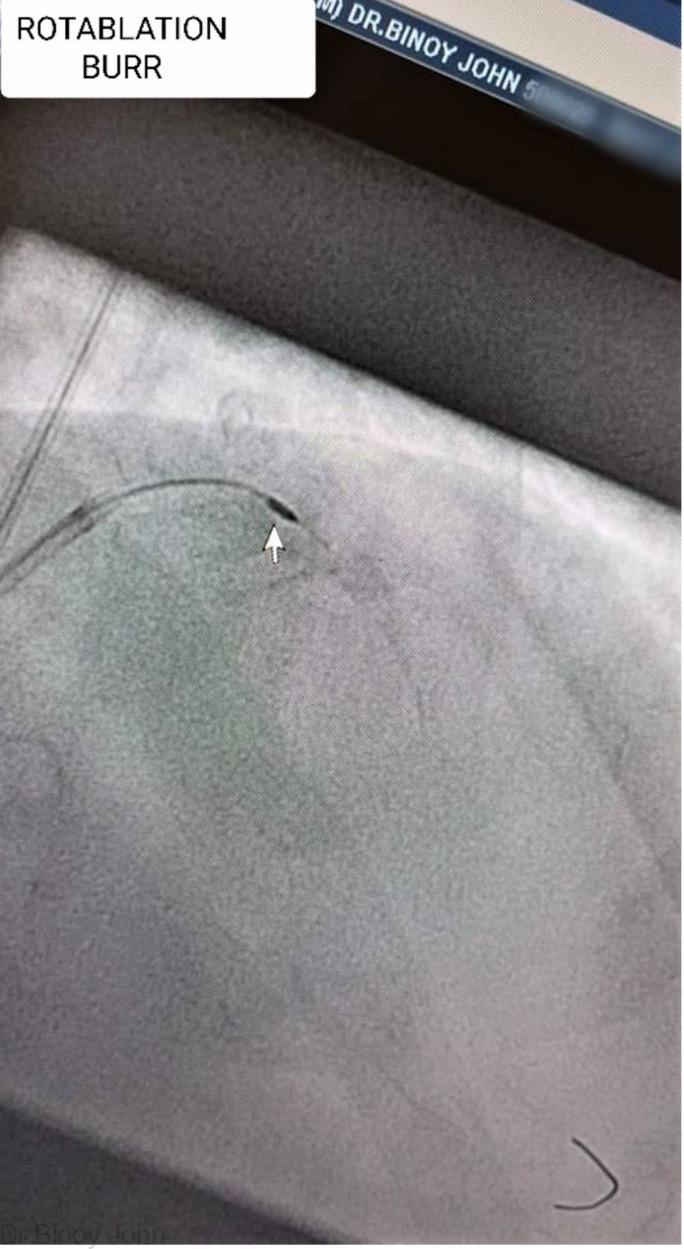
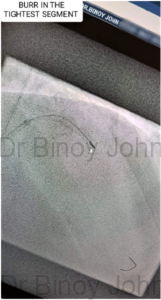
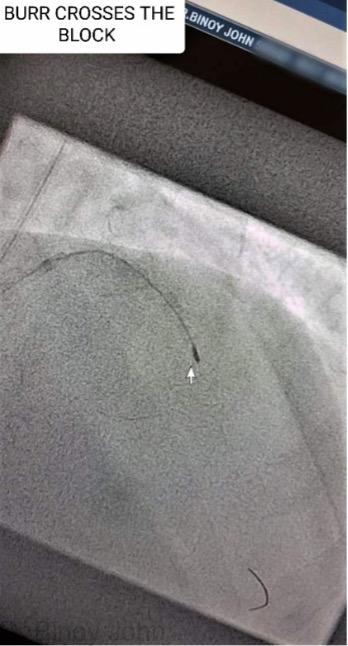
Rotablation angioplasty essentially uses the help of an elliptical shaped burr which has got diamonds on its surface (See picture). This burr is used to drill into the stone hard block. This burr is driven by pressurized air from an external source, to rotate at high speed from 100,000 to 200,000 rotations per minute inside the 2 to 4 mm coronary artery, across the calcified block, just like a hole is a drilled on a wall. This burring preferentially removes the calcium and causes micro-fractures in the stone hard block, which makes it easily amenable to opening with a subsequent regular balloon dilatation. The rotablation burrs come in various diameters and they are selected according to the diameter of the artery. Some blocks may need the use of two or three burrs depending on the complexity and density of the calcium distribution and artery diameter.

What happens to the calcium removed by drilling?
The particles that are created by the drilling are much smaller than our red blood cells and are disposed by our normal body mechanisms.
What is done after burring the block?
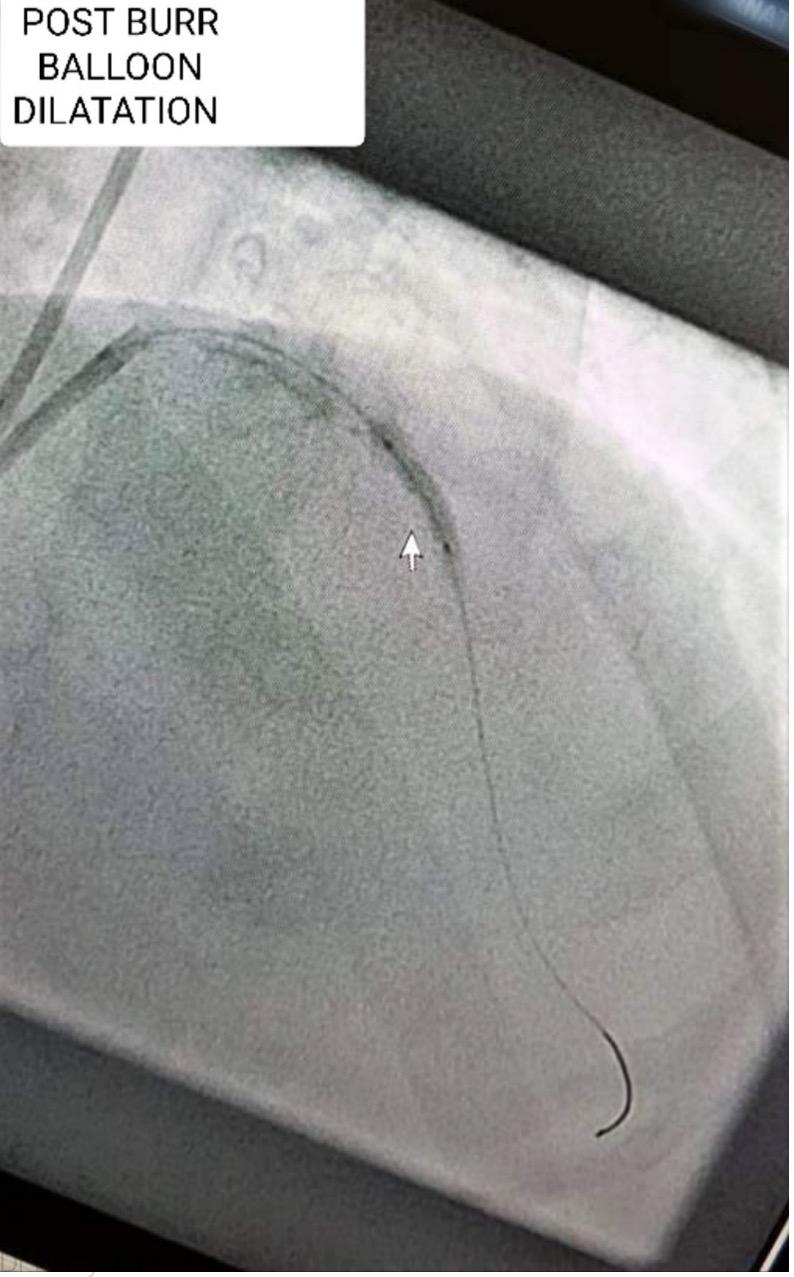
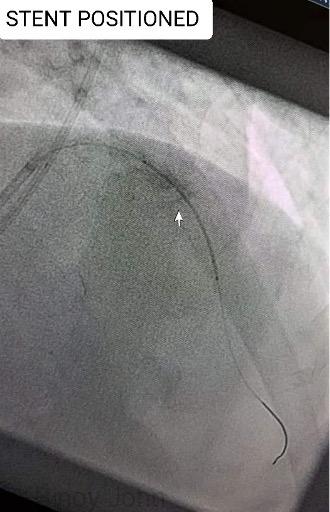
Once a successful rotablation has been done, the subsequent steps are similar to a conventional coronary angioplasty, (See coronary angioplasty) where a balloon is advanced over the wire to open the block. Thereafter a stent is positioned across the block and deployed to prevent a re-block.
Rotablation angioplasty and stenting: Sequential steps of the procedure:

Expertise: Dr Binoy John is an expert in Rotablation angioplasty and has performed numerous rotablation angioplasty including multiple burr rotablations. He has given Tips and trick lectures on Rotablation angioplasty in national and international interventional conferences.
Videos:
- Rotablation in a severely calcified LAD artery
- Rotablation in a high bleeding risk (HBR) patient
- Double burr Rotablation angioplasty
- Tips & Techniques of Rotablation angioplasty





