
What is a Chronic Total Occlusion (CTO) Angioplasty?
Blocks in the, coronary arteries of the heart can sometimes be 100%, which is called total occlusion. Total occlusions can be sudden as when occurs during a heart attack, which then is called an ‘acute’ total occlusion. Angioplasty of a 100% block is called a ‘chronic’ total occlusion (CTO).
Do all Chronic Total Occlusions need angioplasty and stenting?
This is a topic of debate in cardiology. Almost all 100% blocks will have small arterial branches or natural by-pass arteries, called collateral arteries developing in the heart. These collaterals are usually from the other coronary arteries or from the same artery. These collateral arteries supply the portions of the heart muscle which were earlier supplied by the artery which got 100% blocked. (See image) Thus these collateral arteries protect the patient from developing heart-attacks, just like grafts placed during a By-pass surgery. Therefore, due to the collateral supply to the heart muscle, all CTO s often do not need angioplasty and or stenting. An angioplasty is often needed only if that 100% block is producing severe chest pain or breathing difficulty or symptoms which impedes that person’s normal daily routine activities, or if two of the three major arteries are having CTOs and the single open artery is supplying collaterals to the two 100% blocked arteries.
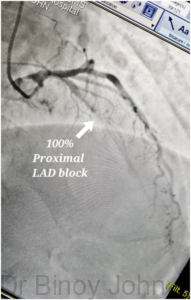
The challenge in a CTO angioplasty:For the success of any angioplasty and stenting the most essential step is to be able to pass a wire across the block. This is because it is only over a wire that a balloon for opening the block and a stent for angioplasty can be delivered to the site of block. If a wire cannot be successfully delivered across a block a balloon or stent cannot be delivered either and therefore an angioplasty will not be possible. (See section: Coronary angioplasty) In a CTO as the block is 100% the region or segment of the artery beyond the 100% block cannot be visualized, making wiring beyond the block challenging as the operator will not know the course of the artery beyond the 100% block. (See image) The Image shows a 100% block in LAD artery seen from forward injection. But, the artery beyond the block cannot be seen, making wiring challenging.
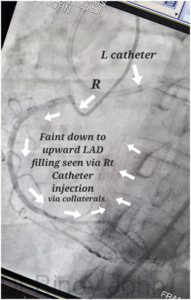
Approach: So, in order to visualize the portion of the artery beyond the 100% block would need the use of collateral dye injection from another artery. The collaterals will fill the portion beyond the block from below upwards, or in a backward flow or retrograde flow. Almost always a dual catheter approach is needed with one catheter to inject dye into the 100% blocked artery and another catheter in the other artery which supplies the collaterals to visualize the terminal end of the 100% blocked artery beyond the 100% block. (See image) The image shows the terminal portion of the 100% LAD seen by dual injection from Right artery, via the collateral arteries.
This dual injection approach helps in safe wiring of the 100% blocked artery. Delivering a wire often can be a forward delivery across the site of 100% block which is called ‘antegrade’ approach or it can be from the reverse end, through another artery via the collateral arteries which is connected to the portion of the 100% blocked artery beyond the 100% block site, called the ‘retrograde’ approach.
Special wires and hardware: Often specialized wires and hardware which are not used in conventional angioplasties are required to perform a CTO angioplasty. Wires with pointed tips and heavy tips may have to be used to penetrate the hard tissue inside the 100% block and cross the block. Often a thin catheter called a micro-catheter will have to be passed into the artery, through which the wire is passedto enable good support and penetrating power for the wire being used. (See image)
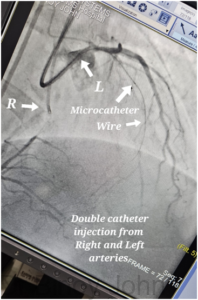
With the help of dual injection of dye from right and left catheters, micro-catheter and specialized wires, often a 100% block can be wired with 70-90% success. (See image)
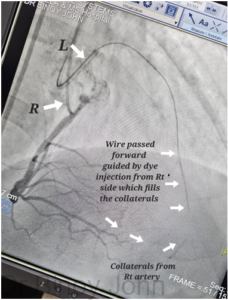
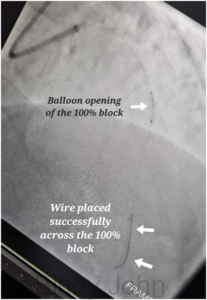
The image shows the successful delivery of a Gaia wire, which is a pointed, heavy wire, across the 100% LAD block with the help of a second catheter dye injection in the Right artery which helps in visualizing the portion of the LAD artery beyond the 100% block in LAD via the collateral arteries. (See Image)
Once the wire crosses into the 100% block into the terminal portion of the artery, the wire can be exchanged for a safer wire and the second catheter can be removed. Thereafter, the steps of the angioplasty are the same as for a conventional angioplasty. A balloon dilatation of the 100% block is performed first. (See image)
Sometimes there maybe difficulty in passing the balloon despite crossing the wire, which then has to be managed with more complex hardware and techniques like rotablation, laser and other hardware.
Once balloon is crossed and a successful dilatation is done, a stent is positioned across the block (See image)
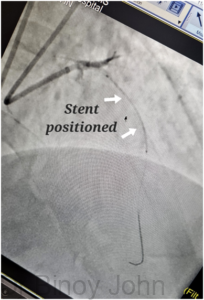
and deployed to get a good flow in the artery and completion of the CTO angioplasty and stenting. (See image)

Expertise: Dr Binoy John is highly experienced in the performance of CTO angioplasty and stenting, when required and believes that all CTO do not need angioplasty and stenting.
Video testimonials:





